



Case of the month: Heaviness of arm in an elderly female with long standing diabetes mellitus !
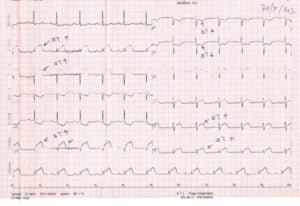
| Clinical scenario : A 76 yr old female complained of heaviness of her left arm and some discomfort on right side of chest. The pain was mild and severity was just 1/10 and it was not associated with diaphoresis . There was no history of shortness of breath , dizziness or palpitations . She has been diabetic for last 20 years on oral hypoglycemic drugs .There was no history of Hypertension and her Lipid estimation few months back were normal . No family history of sudden death or coronary events . Examination: She was conscious oriented .Pulse was 72/min regular , synchronous with other pulses and there was no radiofemoral delay. The volume was good and it had no special character . Her JVP was not elevated .There was no pallor or lymphadenopathy Chest : Trachea was central , movements of the chest were normal and on persuasion there was no dullness . Bronchovesicular breathing was heard without any added sounds. CVS: S1 and S2 were normally heard and there was no gallop or pericardial rub Abdominal examination was normal . CNS : Normal Evaluation : Her Hemoglobin levels were 14gm/dl .She had normal WBC and platelet counts. Her routine ECG showed Fig 1 ST segment elevation in leads II, III, and AVF (Inferior leads )
There is also elevation of ST segment in leads V5 and V6 fig 2 (Lateral leads) and ST depression in V1 and V2 (posterior leads )
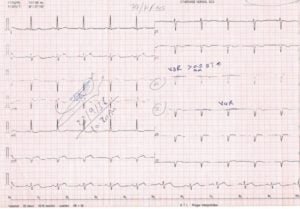
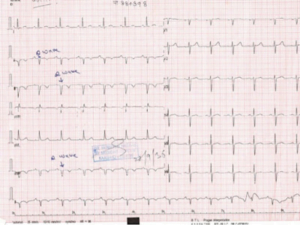
Then ECG of right ventricular Leads was taken which showed ST elevation in V3R and V4R (Fig 2).She had Positive Troponin I .The final diagnosis was Acute inferoposterolateral myocardial infarction with right ventricular extension. She was managed in coronary care unit as acute Myocardial infarction Killip class I (Click to read Killip classification) .She was given loading dose of Tab Aspirin and Clopedogril and Alteplase thrombolysis was started Click to read detailed information about thrombolysis Within half an hour her pain settled and the repeat ECG after thrombolysis is shown in Fig 3
There is Qs with T wave inversion in inferior leads II,III,AVF .There is no more ST elevation in lateral leads and no ST depression in posterior leads She was taken up for coronary angio few days after . Further Reading: Myocardial infarction This case was Contributed by : Consultant Cardiologist King Abdul Aziz Specialist Hospital Taif Saudi Arabia |
Join the mailing list!
Get the latest articles delivered right to your inbox!
