


He had wrongly attributed his low back ache to a trivial fall !
This case was contributed by
Prof Husni Farah
Al – Ahliyya Amman University
Faculty of Medical Sciences
Amman ,Jordan
CLINICAL SCENARIO :
A 66-year-old man presented with sharp, constant, low back pain, dating from a fall from a ladder 6 weeks prior to the current presentation .There was no history of altered sensorium or weakness of any side of his body after he fell from the ladder .He also denied bowel or bladder involvement and was doing activities of daily life routinely . He was attributing his low back ache to the fall .On direct questioning, he did admit to vague malaise for over 6 months.
EXAMINATION:
He was in considerable pain but otherwise seemed fairly fit. He was mildly anemic but had no lymphadenopathy, jaundice or fever. There were no signs of bruising, no deformity of the back and straight leg raising test was negative . Systemic examination was normal as well.
INVESTIGATIONS:
He had haemoglobin levels of 10 .2g/l , white-cell count was normal (6.2 x 109/l). He had a normal differential white-cell count and a normal platelet count but his ESR was 98mm/h. His high ESR was a clue to something underlying.
Total serum proteins were raised at 98g/l (normal 65-75g/l). His serum albumin, creatinine and urea were normal. He had a raised serum calcium level 12.8 mg/dl but normal alkaline phosphatase. Hypercalcemia workup was carried out .
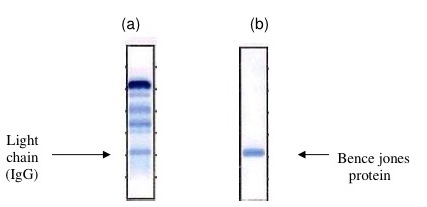 |
| Fig 1 (a) Serum Electrophoresis showing light chains IgG and (b) Urine electrophoresis showing Bence Jones proteins |
Serum protein electrophoresis revealed a monoclonal band in the gamma region (as seen in the figure (1) , with considerable immunosuppression of the rest of this region.
The band was typed by immunoelectrophoresis and shown to be IgG of kappa type Quantitation of serum immunoglobulins showed a raised IgG of 67g/l (normal= 7.2-19.0g/l),
a low IgA of 0.3g/l (NR 0.8-5.0g/l), and a low IgM of 0.2g/l (NR 0.5-2.0g/l).
Electrophoretic examination of concentrated urine showed a monoclonal band in the beta region. On immunoelectrophoresis, this band was composed of free kappa light chains. X-rays of his back showed a small, punched-out lesion in the second lumbar vertebra . He was diagnosed as multiple myeloma and was started on chemotherapy .
Paraproteins
They are found in multiple myeloma disorders and may arise from any of the immunoglobulin classes. Monoclonal light chains are produced in 50% of myeloma and in only 15% heavy chains are found. Increased amount of light chain protein (monoclonal) is excreted in urine as Bence jones protein of type λ. In this case, urine electrophopresis shows very sharp band at the γ- region as seen in Figure 2
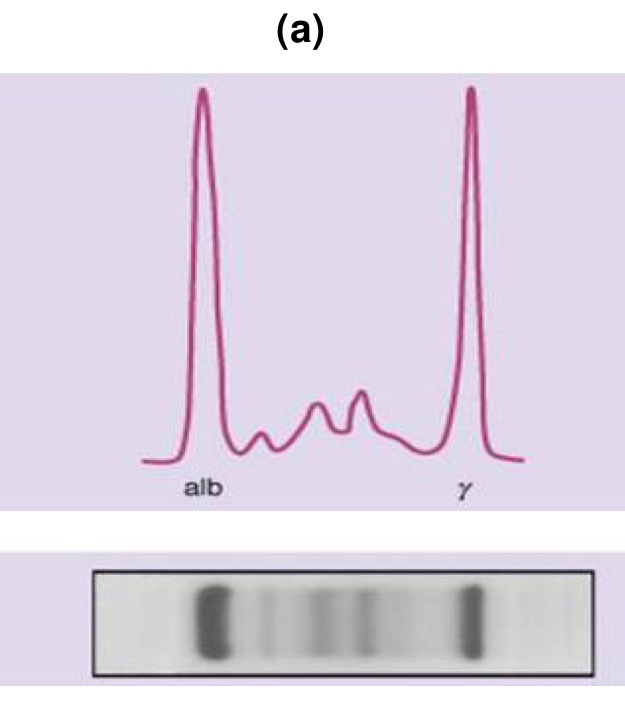 |
| Fig 2 Classical M type of protein band in Multiple myloma |
Multiple myeloma is characterized by production of IgG antibodies, bony metastasis, bone pain especially in skull and in both backbone and pelvis, there is a decreased synthesis in the red blood cells, white blood cells and platelets. Therefore, anemia and recurrent infection are the consequences that appear in this case. In addition, the concentration of Ca+2 is increased in plasma due to the release of Ca+2 from bones.
Hypogammaglobulinemia
At birth, IgM, IgA levels are found decreased, and they start to increase in childhood period. IgA may not reach normal until age 10. During pregnancy, IgG is usually transported through placenta to the fetus. IgG is found increased at birth, then it declines, and rise up again at age 1 year. Any defect in these trends may cause hypogammaglobulinemia.
In a gammaglubulinemia as in Bruton,s disease there is a complete absence of immunoglobulins in plasma whereas in dysgammaglobulinemia there is a partial defect in the synthesis of one or two immunoglobulins type. The levels of immunoglobulins may be reduced in Chronic lymphatic leukemia, Multiple myeloma and Hodgkin,s disease. In addition, chemotherapy (cytotoxic drugs) and nephrotic syndrome cause reduction in the level of immunoglobulins.
Benign paraproteinemia
When there is an increased level of immunoglobulins, the following criteria can be used for the diagnosis of benign paraproteinemia:
a. The clinical features of myeloma do not exist.
b. The immunoglobulins levels are normal.
c. The bones features are normal on radiology.
e. Urine is free from Bence jones protein.
f. The concentration of the light chain protein is less than 10g/L.
Waldenstrom,s Macroglobulinemia
In this defect, the level of IgM is highly elevated causing hypersensitivity and aggregation of RBC in small capillaries in form of thrombosis.
Franklin,s Disease
Increased synthesis of heavy chain protein, which is characterized by malabsorption due to infiltration of gut by malignant cells.
Join the mailing list!
Get the latest articles delivered right to your inbox!