




Case of the month : Where did the Gallstones go?
Clinical scenario:
An 88-year-old male with no comorbid illness presented to the emergency department , with chief complaints of postprandial fullness and on-and-off vomiting of one month duration.
One year back he had developed pain abdomen and was diagnosed to have cholecystitis Ultrasound at that time showed two gallstones without biliary dilatation . He had been managed at a local hospital and discharged home .
The patient denied having had any abdominal surgery or endoscopic procedure prior to current presentation.
On examination:
The patient was thin built mildly dehydrated with normal vitals. Abdominal examination revealed no surgical scar.There was fullness in the upper abdomen but abdomen was soft, not tender and there was no organomegaly or ascites. succussion splash was positive. Bowel sounds were normal
Systemic exam was unremarkable.
Laboratory investigations revealed a hemoglobin of 14gm/dl , white cell and platelet count were normal .The patient had features of pre-renal azotemia which normalized after fluid therapy.
His liver function tests were normal too. After an overnight fast and Ryles tube aspiration an upper GI endoscopic examination was done.Endoscopy revealed evidence of retained liquid in the stomach despite of overnight fast and approximately 1200 ml of fluid was aspirated. A tight stenosis was noted at the pylorus. Only a pediatric diagnostic scope could successfully negotiate the pylorus. The duodenal bulb was deformed, inflamed, and stenotic. An opening was noted at the junction of the duodenal bulb and the second part of the duodenum, with the ampulla lying in very close proximity to this opening. (Fig. 1)
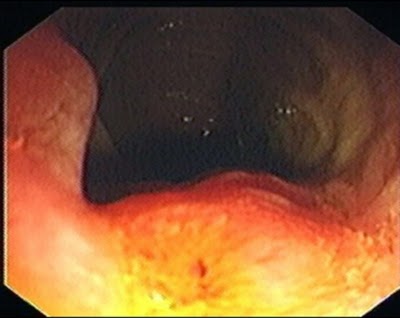 |
| Fig 1 Endoscopy showing opening in duodenal area |
Later CT scan abdomen was done which revealed pneumobilia i.e air in biliary tract, shown as black area under liver (Fig 2 )All other organs were normal and there was no evidence of malignancy
No gallstones .Where did the gallstones go ? where from air came without any intervention or surgery ???
 |
| Fig 2 CT scan abdomen showing air in biliary tract Black shadow under liver above |
Management :
The patient was managed with intravenous omeprazole 80 mg IV stat followed by an 8mg/hour infusion for 3 days. He was gradually started on liquid diet and oral esomeprazole 40mg twice daily, which was continued for another 3 months. The patient was continued on liquid diet, which was later advanced to soft diet with good tolerance.
Repeat endoscopy (EGD) after 10 weeks showed no food residue and the pyloric channel this time permitted an adult diagnostic EGD scope. A catheter was introduced through the previously visualized opening of the choledochoduodenal fistula,(Fig 3) .
 |
| Fig 3 Canulation done to through the opening in duodenum |
The cholangiogram showed dilated common bile duct and intrahepatic biliary ducts (Fig 4) without any filling defect.The gallbladder was distended without any filling defect. This opening only permitted access into the bile duct confirming the fistulous tract between gallbladder and duodenum.
 |
| Fig 4 Cholangiogram obtained and shows the biliary tract . |
So the gallstones had passed from gallbladder into duodenum through this fistulous tract .
In 1896 Léon Bouveret described the first case of gastric outlet obstruction like this due to migration of gallstones and later number of cases were reported in the literature .
The clinical course of acute gastric outlet obstruction, presence of choledochoduodenal fistula, and resolution of symptoms named after Bouveret is called Bouveret’s syndrome.
Message :
Bouveret’s syndrome should be suspected in old debilitated persons with de-novo pneumobilia. Management is surgical or endoscopic . Spontaneous resolution of gastric outlet obstruction in a set of patients may be achieved by proton pump inhibitors without any endoscopic or surgical intervention.
Further reading :
Bouveret’s Syndrome. Case Report and Literature Review
Join the mailing list!
Get the latest articles delivered right to your inbox!

