




Bleeding manifestation of B12 deficiency
A 16-year-old female from a poor socioeconomic status with no known medical illness was admitted with hematemesis, melena of 2 days duration with no history of jaundice or similar illness in the past.
She was a thin built girl with gross pallor,pulse of 130 beats/min and blood pressure (BP) of 90/ 60 mmHg. She had petechial hemorrhages on arms and on legs. Her cardiovascular examination revealed hemic functional murmur in the 5th intercostal space and her other systemic examination was normal .
Evaluation :
On evaluation she had hemoglobin of 2.3 g/dl, leucocytic count of 1000/ml, platelet count 8000/ml, mean corpuscular volume (MCV) 110 fl.
Peripheral smear showed macrocytosis with Howel-Jolly bodies, ovalocytosis and pokilocytosis; platelets were markedly reduced. fig 1
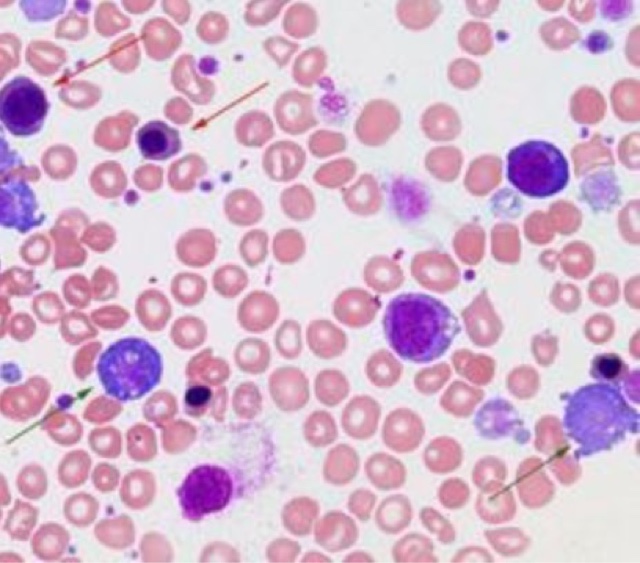 |
| Fig 1 Peripheral blood film of the patient showing Megaloblastosis |
Her serum B12 levels were less than 100 pg/dl (ref. 222– 960 pg/dl) and folate levels were 3.2 ng/dl (3–17 ng/dl). Serum lactate acid dehydrogenase (LDH) levels were high at 1330 U/l. She had normal renal and liver function tests.
After initial resuscitation and transfusion with 3 units of packed red blood cells, her endoscopic examination revealed normal esophagus and there were multiple petechial spots in the body of the stomach, no ulcers, and the duodenum was normal.
Her celiac profile and anti- parietal cell antibody were negative. Stool examination revealed no ova or parasites. Bone marrow examination revealed megaloblastic anemia with myeloid to erythroid ratio (ME ratio) 2 : 1. There was no parasite or infiltration.
She was given therapeutic B12 supplementation (1000 mg daily intramuscular for 7 days), iron and folic acid. supplementation The patient had a marked improvement and her bleeding diathesis stopped.
On the 7th day, her hemoglobin was 9.8 gm/dl, white cell count was 5600/ml and platelet count increased to 1.46000ml. She had retic count of 4%.
The patient was discharged on supplemental vitamin B12, folic acid and iron.
B-12 deficiency may present like hematological malignancy or with bleeding diathesis .
Further reading : click the link Megaloblastic anemia
Join the mailing list!
Get the latest articles delivered right to your inbox!

