



Case of the month: Don’t defer intervention. Delays have dangerous ends: Wellens syndrome Revisited
Contributed by
Dr Parey Mohd Farooq . MD,MRCEM
Emergency medicine Specialist ,University Hospital of Morecambe bay
NHS foundation trust ,United Kingdom
Clinical Scenario
A 63 year old male woke up with substernal chest pain 8/10 ,radiating to left arm associated with mild sweating. The pain lasted for 10 minutes and resolved spontaneously .After an hour ,while walking briskly in the lawn ,he had another episode of Retrosternal Chest pain which was more intense with profuse sweating .EMS were called upon ,arrived within 30 minutes, managed him with Nitroglycerine puffs and Aspirin after which his pain resolved completely
Past medical History Dyslipidemia ,non-compliant to treatment
Heavy smoker -2 packets a day for 15 years
Lives alone ,very fit , tend to exercise regularly
No previous surgical interventions ,No allergies
Drinks occasionally ,denies illicit drug abuse
Clinical Course On arrival to the Emergency department he was clinically asymptomatic .He was hemodynamically stable and denied any Chest pain or Shortness of breath . His was conscious, orientated .His respiratory and cardiovascular exam was unremarkable .He had no lower limb edema A 12 lead ECG was obtained immediately on arrival Fig 1
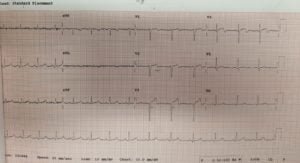
Fig 1 ECG on Arrival
ECG interpretation:;Normal Sinus rhythm , Normal axis Biphasic T waves in precordial leads ,prominent in V2-V4 with terminal negativity .
Subtle STE V3-V4 ,preserved r wave progression , Normal qrs
Initial Troponin = 45 ng/l Normal range <20 ng/l
WBC =6.7 Hb=146 ,Platelets =206 , Na=137,K=4,5
X Ray chest-normal lung fields ,normal cardiac silhouette
Bedside echo : No regional wall motion abnormality
Hospital course
With the clinical impression of Wellens syndrome cardiology referral was done & recommendation of early cardiac catheterisation was discussed accordingly As per cardiology recommendations he was admitted as Acute coronary syndrome under NSTEMI pathway .
It was decided that due to absence of active chest pain ,he wouldn’t be a candidate for emergent cardiac catheterisation .
Treatment with Aspirin ,clopidogrel & Fondaparinux was initiated accordingly .Telemetry was requested and he remained stable and asymptomatic .
Two hours later while awaiting for a bed in CCU patient developed intense substernal chest pain 10/10 radiating to both shoulders .
He was feeling short of breath and sweating profusely .He was immediately shifted to the resus room ,attached to cardiac monitor & pads were placed accordingly .
His blood pressure was 178/98 ,hr=76 , Spo2 was 97 % from air .
A 12 lead ECG was obtained .Fig2 below
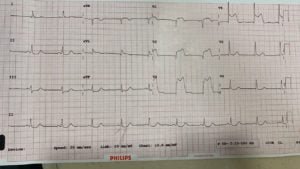
Fig 2 ECG 2hrs later
Anteroseptal Myocardial infarction with St elevation in V1-V4 with inferior reciprocal depression ….
STEMI pathway was activated and patient was immediately transferred for cardiac catheterisation . Coronary angio revealed 95% stenosis of proximal LAD which was successfully treated with drug eluted stent accordingly .He was discharged in good condition and is currently doing well
Teaching message in the case
Wellens syndrome is a specific ECG pattern associated with clinical signs .It’s not a just an ECG findings
The Diagnostic criteria for Wellens syndrome are 1. history of cardiac chest pain, 2.biphasic T waves in V2-V3 (extending to V5-V6) with terminal negativity and/ or 3.deep T wave inversions, with preserved R wave progression in precordial leads and normal to minimally elevated Troponin
There are two different types of T wave patterns and they are seen with complete resolution of pain
-Its considered a warning sign and signifies critical proximal LAD occlusion
-Early cardiac catheterisation is indicated to improve mortality and morbidity
-Its mostly seen in anterior leads however similar pattern has been described in inferior and lateral leads
View in browser :The Health Guide
Join the mailing List of The Health Guide
Join the mailing list!
Get the latest articles delivered right to your inbox!
